WHAT IS DEMENTIA?
Dementia, as defined by the World Health Organisation (WHO), is usually of a chronic or progressive nature, in which there is deterioration in cognitive function beyond what might be expected from normal ageing. It affects memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgement. In Australia, it is the greatest cause of disability in adults over the aged of 65. One in 10 people over the age of 65, and three in 10 people over the age of 85 is estimated to have dementia. In the residential aged care setting, people with dementia accounts for about 52% of all residents.
WHAT ARE DIFFERENT TYPES OF DEMENTIA?
ALZHEIMER’S DISEASE
Alzheimer’s Disease is the most common type of dementia, it accounts for 60-70% of cases worldwide. It has a gradual onset of symptoms, and is a progressive disease which worsens over time. Symptoms include deficits in memory, impaired language comprehension, difficulties in speech production, dysfunction in visual and spatial awareness, and psychological and behavioural changes. Alzheimer’s Disease is characterised by deposits of toxic peptide between neurons causing disruption in normal brain function, as well as tangles in the neuron structure, causing disruption in the transportation of energy and nutrients to the neurons, leading to cell death and brain atrophy.
VASCULAR DEMENTIA
Vascular dementia is the second most common cause of dementia. Although there are many different types of vascular dementia, they are all characterised by impaired blood supply to the brain. Typically, there is an abrupt onset of symptoms, followed by a progressive step-wise decline. Vascular dementia is preceded by effects of vascular disease, which involve damage to the blood vessels leading to reduced blood flow to the brain. The reduction of blood flow deprives neurons of nutrients and oxygen, leading to cell death and brain atrophy. This usually occurs in the areas of the brain responsible for memory, thinking and language, and lead to cognitive deficits.
Vascular dementia can be classified into four different types:
- Sub-cortical ischemic vascular dementia – occlusion of small blood vessels deep in the brain.
- Cortical dementia – pathologies in the cerebral cortex.
- Post-stroke/multi-infarct dementia – series of small strokes following a large stroke.
- Mixed dementia – combination of Alzheimer’s disease and vascular dementia
LEWY BODY DEMENTIA
Lewy body dementia is linked with abnormal protein deposits that accumulate inside neurons at the pre-synapse in the brain, forming ‘Lewy bodies’. This type of dementia is rapid. Unlike Alzheimer’s Disease, memory deficits are usually affected later on, and it usually affects the semantic memory which is responsible for recollection of general facts/concepts.
There are three core features of dementia with Lewy bodies:
- Parkinsonism
- Fluctuating cognition
- Visual hallucinations
FRONTOTEMPORAL DEMENTIA
Frontotemporal dementia is the least common type of dementia. It affects the frontal and temporal lobes of the brain. As a guideline, impairments to the frontal lobe may lead to changes associated with behaviour, personality, whereas impairments to the temporal lobe will lead to language deficits.
There are three different types of Frontotemporal dementia:
- Frontal (behavioural) variant – affecting personality, behaviour and executive function.
- Semantic dementia – unable to identify or understand the meaning of words or concepts.
- Progressive non-fluent aphasia – affecting production of speech and appear non-fluent.
HOW CAN PHYSIOTHERAPY HELP?
Essentially, the role of a physiotherapist in the management of dementia is dependent on the severity of the dementia. Ideally, interventions need to be implemented as early as possible, when the potential for motor learning is at its greatest.
STAGES OF DEMENTIA AND PHYSIOTHERAPY GOALS
The physiotherapy goals for each stage requires consideration of the cognitive and functional capacity of the individual.
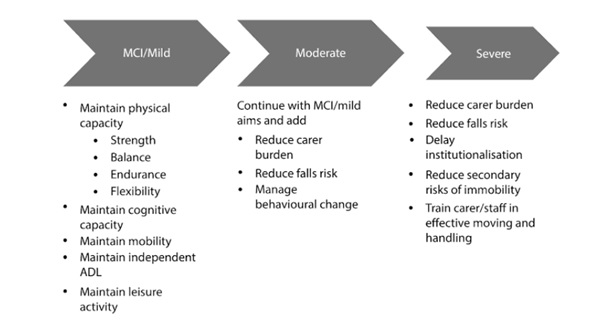
(Lord & Rocheter, 2017)
BENEFITS OF EXERCISE
Numerous literatures exist investigating the positive effects of exercise in the management of dementia. According to research, in addition to improving physical function and reducing risk of falls, exercise also has a protective effect against cognitive decline and reduces risk of cognitive regression. People living with dementia often experience other age-related co-morbidities which may be improved and better managed with exercise (e.g. osteoarthritis, osteoporosis and diabetes). It also promotes better cardiovascular health, which is especially important for those affected by vascular dementia. Physical activity also elevates a persons’ mood by activating the reward and pleasure pathways in the brain, which can reduce the physiological response to stress and improve one’s sense of well-being. Exercise in a group setting may also contribute to feelings of reassurance, and promote active social involvement, which address depression and apathy experienced by many people with dementia.
Written by Lauren Kendall
Physiotherapy Student
REFERENCES
Cadore, E. L., Moneo, A. B. B., Mensat, M. M., Muñoz, A. R., Casas-Herrero, A., Rodriguez-Mañas, L., & Izquierdo, M. (2014). Positive effects of resistance training in frail elderly patients with dementia after long-term physical restraint. Age, 36(2), 801-811.
Garcia-Esparcia, P., López-González, I., Grau-Rivera, O., García-Garrido, M. F., Konetti, A., Llorens, F., … & Gelpi, E. (2017). Dementia with Lewy bodies: molecular pathology in the frontal cortex in typical and rapidly progressive forms. Frontiers in neurology, 8, 89.
Haider, A., & Dulebohn, S. C. (2018). Dementia, Lewy Body.
Hughes, J. C. (2011). Alzheimer’s and other Dementias. Oxford University Press.
Jenkins, C., Ginesi, L., & Keenan, B. (2015). Dementia care at a glance. John Wiley & Sons.
Kosaka, K. (2017). Dementia with Lewy bodies. Current opinion in neurology, 9(4), 271-275.
Kumar, A., & Singh, A. (2015). A review on Alzheimer’s disease pathophysiology and its management: an update. Pharmacological Reports, 67(2), 195-203.
Lleo, A., & Blesa, R. (2017). Pathophysiology of Alzheimer’s disease. In G. Waldemar & A. Burns (Eds.), Alzheimer’s Disease (pp. 24-34). Oxford University Press.
O’Brien, J., & Thomas, A. (2015). Vascular dementia. The Lancet, 386(10004), 1698-1706.
Roh, J. H., & Lee, J. H. (2014). Recent updates on subcortical ischemic vascular dementia. Journal of stroke, 16(1), 18.
Scherder, E., Eggermont, L., Swaab, D., van Heuvelen, M., Kamsma, Y., de Greef, M., … & Mulder, T. (2007). Gait in ageing and associated dementias; its relationship with cognition. Neuroscience & Biobehavioral Reviews, 31(4), 485-497.
Schwenk, M., Zieschang, T., Englert, S., Grewal, G., Najafi, B., & Hauer, K. (2014). Improvements in gait characteristics after intensive resistance and functional training in people with dementia: a randomised controlled trial. BMC geriatrics, 14(1), 73.
Sherrington, C., & Tiedemann, A. (2015). Physiotherapy in the prevention of falls in older people. Journal of physiotherapy, 61(2), 54-60.
Warren, J. D., Rohrer, J. D., & Rossor, M. N. (2013). Frontotemporal dementia. Bmj, 347, f4827.
World Health Organsiation. (2018). Dementia. Retrieved from https://www.who.int/news-room/fact-sheets/detail/dementia