Hip protectors are commonly prescribed in the Residential Aged-care Facilities (RACFs) by doctors, physiotherapist, nurses and other health professions. For many facilities, hip protectors are utilised as ‘first-line of defence’ in prevention of hip fractures and provided to every resident following a fall. However, how much do we really know about hip protectors and its effectiveness in preventing fractures?
Falls & Hip Fractures:
About one third of people aged 65 and over will have a fall each year. Rate of fall is substantially higher among older adults living in RACFs. Around 1~2% of falls will result in a hip fracture, and it is one of the most severe injuries for an elderly individual as major surgery and extensive rehabilitation is required. More than 90% of all hip fractures are sustained as a consequence of a fall, and females are 80% more likely to sustain a hip fracture than males.
Hip fractures have a dramatic impact on an individual’s quality of life. It leads to reduced mobility, lost of independence, risk of social isolation and increase risk of secondary health complications. Furthermore, the mortality rate for an elderly person following a hip fracture is ~10% at 1 month, ~30% at one year, and only ~50% regain pre-morbid function. This makes preventing falls and hip fractures central components in the care of the residents in RACF.
Using Hip Protectors:
Hip protectors are undergarments with protective material over the hip region which either absorb or disperse the force acting on the hip during the impact of a fall. There are two types of protective material; hard shields which divert energy away from the hips toward the surrounding tissue, and soft pads which absorbs the energy from impact.
Numerous studies have attempted to determine the effectiveness of hip protectors in preventing hip fractures. However, many studies were plagued with poor quality and compliance issues. In a systematic review conducted by Santesso et al (2014), it was found that residents wearing hip protectors at time of a fall are ~18% less likely to sustain a hip fracture in an institutional setting. It was also found that hard shield, which diverts energy away from the hip, are more effective in preventing hip fractures than soft pads which absorbs energy.
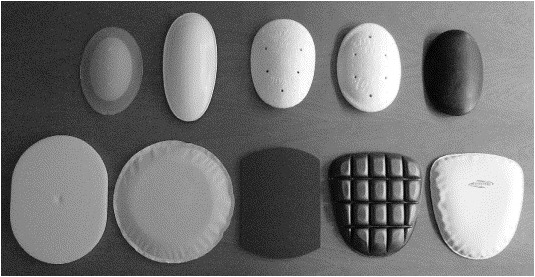
Top row: Examples of hard shields in hip protectors.
Bottom row: Examples of soft pads in hip protectors.
Factors Affecting Hip Protector Use:
The single most significant factor impacting the use of hip protectors is user compliance. Various studies reported low compliance which may have impacted the results. Issues such as comfort, practicality, extra effort, and cost contributed to low compliance levels. Use of hip protector is largely affected by resident’s motivation to wear, and attitude of care staff members towards its use. In the systematic review by Santesso et al (2014), soft pads has been found to have higher rate of compliance compared with hard shields, predominately due to superior user comfort.
Other Considerations for Preventing Fractures:
Osteoporosis Management:
Osteoporosis is characterised by reduced bone density and health. Currently, there are no management strategies that can normalise bone density. However, small improvement in bone density has proven to reduce risk of fractures. There is evidence indicating under-treatment of Osteoporosis in RACFs, especially for resident at risk of, or has history of fractures, which makes Osteoporosis management a key component is fracture prevention. Studies have shown beneficial effects of Biphosphonates, Selective Oestrogen Receptor Modulators, and Strontium Renelate, in prevention of fractures for postmenopausal women diagnosed with osteoporosis and low bone density.
Vitamin D:
It is found that vitamin D supplement reduces the risk of falls among residents with stable health by ~20%. It is unclear how exactly vitamin D acts to reduce risk of falls. One potential rationale is its positive effect on muscle function. Vitamin D from dietary intake is has been shown to be insufficient, especially for residents in RACFs. Residents can obtain more vitamin D through supplements, which is often coupled with calcium, and being exposed to sunlight (main source of vitamin D).
Conclusion:
In summary, prevention of falls and hip fractures is multi-factorial. The evidence has demonstrated mild effectiveness of hip protectors in preventing hip fractures for residents in RACFs. However, studies were impacted by poor compliance from participants, which is a consistent issue in the real-world RACF setting. Although hard shield hip protectors were found to be more effective, soft pads has been widely used as it showed better compliance among users due to superior comfort. Discussion with residents and care staff education is a vital component to improving compliance of hip protector use. Other Elements such as osteoporosis management, and vitamin D & Calcium supplement should be considered in prevention of hip fractures.
Recommendation for Hip Protector Use:
- Consider resident’s falls history, age, mobility status, disability, cognition & BMI when prescribing hip protectors.
- Include resident and family in discussion of hip protector use to improve compliance.
- Ensure appropriate fitting (size & position) of hip protectors to optimise comfort for resident.
- Educate staff on importance of hip fracture prevention and appropriate fitting of hip protectors.
- Support & encourage resident in hip protector compliance.
- Consider & review osteoporosis management medications as well as vitamin D & calcium supplements.
- Consider & review additional falls prevention strategies.
Contact us here at ProActive Care to find out more about hip protectors and how we can help with preventing falls and hip fractures.
Written by Ian Lai & Henry Kuo
ProActive Care – Physiotherapists
References:
Australian commission on safety and quality of health care https://www.safetyandquality.gov.au/our-work/falls-prevention/
Bentzen H, Bergland A, Forsen L (2008) ” Risk of hip fractures in soft protected, hard protected, and unprotected falls [with consumer summary]”. Injury Prevention Oct; 14 (5): 306-310
Oliver D, Connelly JB, Victor CR, Shaw FE, Whitehead A, Genc Y, et al. Strategies to prevent falls and fractures in hospitals and care homes and effect of cognitive impairment: systematic review and meta-analyses. BMJ 2007;33 4(7584): 82. MEDLINE: 17158580
Santesso N, Carrasco-Labra A, Brignardello-Petersen R (2014) “Hip protectors for preventing hip fractures in older people”. Cochrane Database of Systematic Reviews 2014, Issues 3 Art. No.: CD001255
Sawka AM, Boulos P, Beattie K, Papaioannou A, Ga fni A, Cranney A, et al. Hip protectors decrease hip fracture risk in elderly nursing home residents: a Bayesian meta-analysis [Erratum ap pears in J Clin Epidemiol. 2008 Aug;61(8): 854]. Journal of Clinical Epidemiology 2007;60(4):336–44. MEDLINE: 17346606van Schoor NM,
van der Veen AJ, Scaap LA, Smit TH, Lips P (2006) “Biomechanical comparison of hard and soft hip protectors and the influence of soft tissue”. Bone 39 (2): 401-407